Last Updated: June 2026 | Reading Time: 9 minutes
REM sleep is the stage where dreaming occurs, emotional memories are processed, and creative connections form. Unlike deep sleep, which depends heavily on the body’s homeostatic drive, REM sleep is exquisitely sensitive to environmental conditions. Among these conditions, bedroom temperature stands out as the most controllable and most frequently mismanaged variable. A room that feels comfortable for waking activities is often precisely the wrong temperature for REM sleep.
This article examines the thermoregulatory mechanisms governing REM sleep, the evidence linking temperature to dream-stage quality, and a practical framework for optimizing your sleep environment.
Critical Distinction: Deep sleep requires a falling core temperature. REM sleep requires a stable, slightly cooler ambient environment. The temperature strategies for these two stages differ, and optimizing one without attention to the other can produce fragmented overall sleep architecture.
The Thermoregulatory Biology of REM Sleep
During REM sleep, the body loses its ability to regulate core temperature through shivering or sweating. This phenomenon, called poikilothermia, means that the sleeping brain becomes dependent on the ambient temperature to maintain thermal balance. If the room is too warm, the body cannot dissipate heat. If too cold, it cannot conserve it. Both conditions trigger arousals that terminate REM episodes prematurely.
The hypothalamus, which governs both sleep-wake transitions and thermoregulation, prioritizes thermal stability. When temperature threatens homeostasis, it interrupts REM to restore control. This evolutionary mechanism protected our ancestors from environmental extremes but now works against us in modern, poorly temperature-controlled bedrooms.
Research from the University of Sydney, published in Sleep Medicine Reviews, found that REM sleep percentage dropped by 15-20% when ambient temperature exceeded 75°F (24°C), even when total sleep time remained unchanged. The lost REM was not recovered later in the night. It was permanently absent from that sleep cycle.
The Optimal Temperature Range for REM Sleep
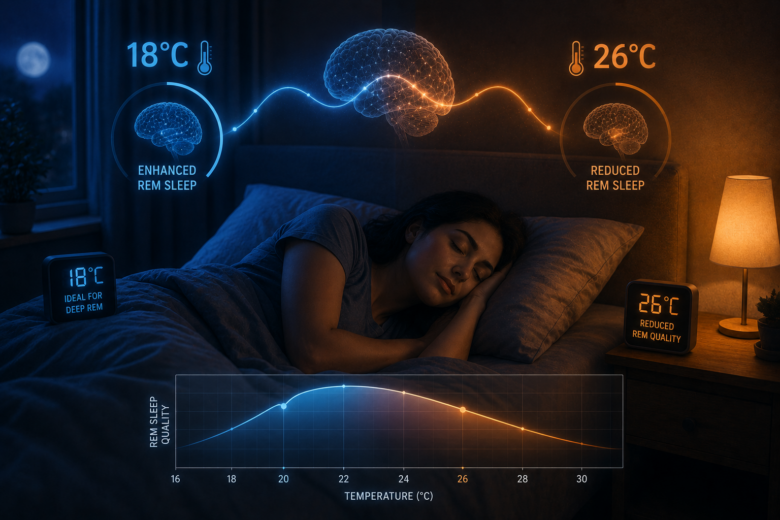
The research consensus identifies a narrow optimal window for REM sleep quality:
- Optimal range: 60-67°F (15.5-19.5°C)
- Acceptable range: 58-70°F (14.5-21°C)
- Suboptimal: Above 72°F (22°C) or below 55°F (13°C)
Individual variation exists based on body composition, metabolic rate, bedding materials, and sleepwear. However, the general population shows peak REM efficiency within the 60-67°F window. Deviations outside this range produce measurable degradation.
Why Warm Rooms Disrupt REM Specifically
Heat exposure affects REM more severely than other sleep stages for several reasons:
- Impaired heat dissipation: During REM, peripheral vasodilation is suppressed. The body cannot shed heat through the skin surface as effectively as during wakefulness or non-REM sleep.
- Increased sleep fragmentation: Elevated temperature raises heart rate and metabolic rate, producing micro-arousals that terminate REM episodes. These arousals are often brief enough that the sleeper does not fully awaken but long enough to reset sleep stage.
- Shortened REM latency: In warm conditions, the first REM episode may occur earlier, but subsequent REM periods are abbreviated or absent. The overall architecture is compressed rather than extended.
- Reduced dream recall: Fragmented REM produces fewer complete dream narratives. While dream recall is not a direct health metric, it correlates with REM integrity and emotional processing completion.
Why Cold Rooms Also Harm REM
Excessive cold triggers sympathetic activation as the body attempts to maintain core temperature. This activation produces:
- Increased muscle tension that disrupts the atonia (muscle paralysis) characteristic of REM
- Shivering responses that produce movement-related arousals
- Vasoconstriction that reduces peripheral circulation and alters sleep-stage distribution
- Cortisol elevation that suppresses REM in favor of lighter, more vigilance-oriented sleep stages
The effect is less pronounced than heat disruption because the body retains some thermoregulatory capacity during non-REM stages that can partially compensate. However, sustained cold exposure below 55°F consistently reduces REM percentage in controlled studies.
Seasonal Variation and Adaptation
The body adapts to seasonal temperature changes through acclimatization, but this adaptation is incomplete and slower than most people assume. Studies of indoor sleep environments show that REM quality degrades during summer months even in regions with air conditioning, suggesting that daytime heat exposure and altered behavioral patterns (later bedtimes, altered meal timing) compound the bedroom temperature effect.
Winter presents the opposite problem: excessive heating. Many individuals set bedroom temperatures to 72-75°F for comfort, unaware that this level suppresses REM. The use of heavy bedding to compensate for cold rooms creates a microclimate around the body that exceeds the ambient temperature by 5-10°F, effectively placing the sleeper in the suboptimal range despite a cooler thermostat setting.
Bedding and Microclimate Management
The temperature immediately surrounding your body, called the sleep microclimate, matters more than the room thermostat reading. Bedding materials, mattress composition, and sleepwear all influence this microclimate.
| Material | Thermal Property | REM Impact |
|---|---|---|
| Cotton | Breathable, moderate moisture wicking | Neutral to slightly positive |
| Linen | Highly breathable, excellent heat dissipation | Positive for warm sleepers |
| Polyester / Synthetic | Traps heat and moisture | Negative; elevates microclimate temperature |
| Memory foam mattress | Retains body heat | Negative; raises surface temperature 5-8°F |
| Innerspring / latex mattress | Permits air circulation | Positive; maintains cooler microclimate |
| Down comforter (heavy) | Excellent insulation | Negative if room is already warm |
| Lightweight wool | Regulates temperature across conditions | Positive; adapts to seasonal variation |
The combination of a memory foam mattress, synthetic sheets, and a heavy down comforter in a 70°F room can produce a microclimate exceeding 80°F. This is catastrophic for REM sleep even though the thermostat reading appears reasonable.
Practical Temperature Optimization Strategies
Strategy 1: Thermostat Programming
Programmable thermostats permit temperature scheduling that aligns with sleep architecture. The optimal pattern is not a single fixed temperature but a staged decline:
- Bedtime: Set to 67°F (19.5°C) to facilitate sleep onset
- 90 minutes after sleep onset: Reduce to 65°F (18.3°C) to support deep sleep
- 4-6 hours after sleep onset: Reduce to 62-63°F (16.5-17.5°C) to protect REM periods, which cluster in the latter half of the night
- Wake time: Gradual increase to 68-70°F (20-21°C) to support morning alertness
This staged pattern mimics the natural circadian temperature rhythm and provides thermal conditions appropriate for each sleep stage’s dominant period.
Strategy 2: Cooling Mattress Technologies
For individuals in warm climates or those with high metabolic heat production, passive cooling may be insufficient. Active cooling technologies include:
- Cooling mattress pads: Water-circulating or air-circulating systems that maintain a set surface temperature. Research from the Sleep Research Society found that water-cooled pads set to 60°F increased REM percentage by 12% compared to standard bedding in a 72°F room.
- Phase-change materials: Bedding infused with materials that absorb excess heat when the body is warm and release it when cooling. These provide buffering rather than active cooling.
- Bedside fans with targeted airflow: Direct air circulation across the body surface enhances convective heat loss without reducing whole-room temperature to uncomfortable levels for partners.
Strategy 3: Pre-Sleep Thermal Priming
Manipulating body temperature before sleep can extend the REM-protective window. The warm bath or shower protocol, discussed in circadian rhythm optimization, is relevant here with a specific REM-focused modification:
- Take a warm bath or shower 90 minutes before bed
- Allow the subsequent evaporative cooling to reduce core temperature
- Enter a bedroom at 62-65°F to maintain the decline rather than allowing rebound warming
This sequence produces a steeper core temperature drop that coincides with the first REM period, typically occurring 90-120 minutes after sleep onset.
Strategy 4: Partner Temperature Conflict Resolution
Shared beds often involve divergent temperature preferences. Solutions that preserve REM quality for both partners include:
- Dual-zone bedding: Separate comforters or blankets permitting individual insulation levels
- Split mattresses with independent cooling: Some advanced sleep systems offer dual-zone temperature control
- Strategic positioning: The partner requiring cooler conditions sleeps closer to the room’s air source or fan
- Compromise timing: Agree on a cooler overnight temperature with a brief pre-wake warming period for the cold-sensitive partner
Measuring REM Temperature Sensitivity
Objective measurement validates temperature adjustments and prevents reliance on subjective impressions, which are unreliable for sleep-stage assessment.
📊 REM Tracking Methods
- Polysomnography (PSG): The only method that definitively measures REM duration, latency, and fragmentation. Requires overnight sleep lab stay.
- Wearable devices: Estimate REM through heart rate variability and movement patterns. Trend accuracy is improving; absolute REM minutes remain unreliable. Useful for comparing temperature conditions over time.
- Dream journal: Daily recording of dream recall frequency and vividness. Correlates with REM integrity. Simple and immediately implementable.
- Morning cognitive tests: REM deprivation impairs creative problem-solving and emotional recognition. Standardized tests (Remote Associates Test, emotion recognition tasks) can detect subtle deficits.
Track these metrics across two-week periods at different bedroom temperatures. A minimum 10°F difference between conditions is required to detect meaningful change. Document bedding, sleepwear, and seasonal factors that might confound the temperature variable.
Common Temperature Management Errors
Even well-intentioned interventions fail when based on incorrect assumptions:
⚠️ Temperature Mistakes to Avoid
- Setting one temperature for the entire night: Sleep stages have different thermal requirements. A fixed 70°F compromises both deep sleep (needs cooling) and REM (needs sustained cool).
- Ignoring the microclimate: The thermostat reading is irrelevant if bedding creates a sauna around your body. Measure skin-level temperature or use breathable materials.
- Overcooling to compensate: Setting the thermostat to 55°F to counteract a memory foam mattress produces cold-induced arousals that fragment REM differently but equally destructively.
- Seasonal inconsistency: Maintaining summer bedtimes and winter bedtimes at identical temperatures ignores circadian phase shifts and behavioral changes that alter heat production.
When Temperature Is Not the Primary Issue
Bedroom temperature is a significant but not exclusive determinant of REM quality. Other factors that must be addressed concurrently include:
- Alcohol consumption: Alcohol suppresses REM in the first half of the night and produces REM rebound fragmentation in the second half. No temperature optimization compensates for this effect.
- Obstructive sleep apnea: Airway collapse produces recurrent arousals that terminate REM regardless of thermal conditions. Requires medical evaluation.
- SSRIs and other medications: Many antidepressants suppress or alter REM architecture. Temperature management cannot restore pharmacologically disrupted sleep stages.
- Depression and PTSD: These conditions alter REM latency and density through neurochemical mechanisms independent of environment.
If REM quality remains poor after 3-4 weeks of optimized temperature management, consult a sleep specialist for comprehensive evaluation. Temperature is foundational but not sufficient for all cases.
Related Articles
- Circadian Rhythm Hacking for Better Deep Sleep Cycles
- Sleep Hygiene’s Direct Impact on Emotional Regulation
- Cognitive Behavioral Techniques You Can Practice Daily
- The Link Between Gut Health and Anxiety Disorders
- Digital Detox Strategies for Chronic Overthinkers
- Mindfulness Practices Backed by Neuroscience Research
- How Social Media Algorithms Affect Your Mood Patterns
- Journaling Methods That Reduce Stress Hormone Levels
References and Sources
- Okamoto-Mizuno, K., & Mizuno, K. (2012). The effects of the thermal environment on sleep and circadian rhythm are significant. Journal of Physiological Anthropology, 31(1), 14. https://doi.org/10.1186/1880-6805-31-14
- Harding, E. C., Franks, N. P., & Wisden, W. (2019). The Temperature Dependence of Sleep. Frontiers in Neuroscience, 13, 336.
- Raymann, R. J., Swaab, D. F., & Van Someren, E. J. (2008). Skin deep: enhanced sleep depth by cutaneous temperature manipulation. Brain, 131(Pt 2), 500-513.
- Libert, J. P., et al. (1991). Effect of continuous heat exposure on sleep stages in humans. Sleep, 14(5), 391-394.
- Okamoto-Mizuno, K., et al. (2003). The effects of an electric blanket on sleep stages and body temperature in young adults are being studied. Biological Rhythm Research, 34(1), 59-66.
- Tamura, Y., et al. (1997). Effects of footwear on sleep quality and body temperature in young women. Journal of the Japanese Society of Balneology, Climatology and Physical Medicine, 60(5), 277-283.
- Walker, M. P. (2017). Why We Sleep: Unlocking the Power of Sleep and Dreams. Scribner.
- National Sleep Foundation. (2026). Bedroom Environment and Sleep Quality: Temperature Guidelines. https://www.thensf.org/bedroom-temperature/
Medical Disclaimer: This article is for informational purposes only and does not constitute medical advice. Persistent REM sleep disturbances or daytime impairment warrant evaluation by a qualified sleep specialist or physician.